Medical image super-resolution (SR) has emerged as a critical technique for enhancing diagnostic capabilities while addressing limitations in imaging hardware, scan time, and patient comfort. This survey provides a comprehensive review of machine learning (ML) and deep learning (DL) approaches for medical image SR, covering classical methods, traditional ML techniques, and state-of-the-art deep learning architectures. We systematically analyze SR methods across multiple medical imaging modalities including CT, MRI, ultrasound, microscopy, and nuclear imaging. Through extensive comparison of network architectures, loss functions, and evaluation metrics, we highlight the evolution from sparse coding and dictionary learning to advanced convolutional neural networks (CNNs), generative adversarial networks (GANs), and vision transformers. We discuss critical challenges including data scarcity, domain generalization, clinical validation, and real-world deployment. Finally, we outline promising future directions including self-supervised learning, federated learning, and explainable AI for medical SR.
Medical imaging has become an indispensable component of modern clinical practice, enabling clinicians to visualize and assess anatomical structures and physiological processes non-invasively. Imaging modalities such as Magnetic Resonance Imaging (MRI), Computed Tomography (CT), Ultrasound, Positron Emission Tomography (PET), and Digital Pathology are integral to disease diagnosis, treatment planning, and clinical decision-making [1]. The diagnostic accuracy of these modalities is directly influenced by image quality, particularly spatial resolution, which determines the ability to visualize fine anatomical details such as microvasculature, lesions, or tissue boundaries.
Despite continuous improvements in acquisition hardware and reconstruction algorithms, medical images are often acquired at limited resolution. Physical and clinical constraints—including scan time, patient motion, hardware limits, and radiation dose—pose significant barriers to high-resolution imaging [4]. In CT imaging, increasing spatial resolution is often achieved at the cost of higher radiation exposure, which may be clinically unacceptable [3]. In MRI, high-resolution scans require longer acquisition times, resulting in patient discomfort, increased risk of motion artifacts, and lower throughput. Ultrasound imaging is fundamentally limited by transducer bandwidth and signal attenuation.
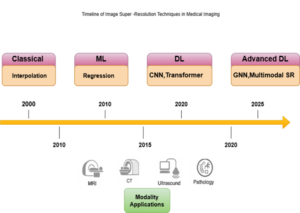
Figure 1. Timeline of medical image super-resolution (SR) techniques, illustrating the progression from classical interpolation and ML regression methods to modern DL and advanced GNN-based multimodal SR approaches across MRI, CT, ultrasound, and pathology modalities.
Numerous studies have demonstrated the clinical benefits of super-resolution (SR). In MRI, SR techniques can enhance tumor visualization and improve volumetric quantification accuracy [7]. In CT imaging, SR can allow for reduced radiation dose while preserving image sharpness [8]. In ultrasound, SR has been applied to improve vascular imaging and microstructure visualization beyond the physical diffraction limit [5]. In digital pathology, SR can help reconstruct gigapixel-level whole-slide images, improving the accuracy of computational diagnosis. These examples highlight how SR can improve both diagnostic confidence and clinical efficiency.
The medical imaging field has increasingly adopted super-resolution (SR) techniques to overcome modality-specific limitations. In MRI, SR has been applied to improve spatial resolution for tumor detection, brain imaging, and functional mapping [5]. In CT, SR can reduce the required radiation dose by reconstructing high-resolution images from low-dose acquisitions [8]. Ultrasound SR enables super-resolved visualization of vascular networks, expanding the utility of non-invasive imaging [6]. In digital pathology, SR enhances image quality for automated analysis tasks such as segmentation and classification.
Despite these advances, several challenges remain. Data scarcity is a persistent bottleneck, as paired low-resolution–high-resolution (LR–HR) datasets are difficult to obtain in clinical settings due to privacy and acquisition constraints [18]. Domain generalization remains limited, as SR models trained on data from one scanner or institution often perform poorly on others. Standard evaluation metrics such as PSNR and SSIM may not correlate well with clinical utility, necessitating task-specific and perceptual evaluation strategies. Furthermore, the interpretability and reliability of deep learning-based SR methods remain active areas of research.
Main contributions of this survey
Although several reviews on super-resolution (SR) exist, few provide a comprehensive, modality-aware synthesis of classical, machine learning (ML), and deep learning (DL) methods specifically tailored to medical imaging. The main contributions of this survey are:
In summary, SR represents a powerful approach to enhancing medical image quality while minimizing acquisition costs and risks. This survey aims to serve as a comprehensive reference for researchers and practitioners at the intersection of medical imaging and artificial intelligence, supporting both methodological innovation and clinical translation.
Image Super-Resolution (SR) refers to the process of reconstructing a high-resolution (HR) image from one or more low-resolution (LR) inputs [19]. The goal is to recover lost high-frequency information, such as edges and fine anatomical details, that are typically degraded during image acquisition. SR is a crucial task in medical imaging, as it enhances the visibility of structures and supports improved diagnosis, image analysis, and computer-aided decision-making [6].
The SR problem is often modeled as an inverse problem. Given an LR image , the objective is to estimate its corresponding HR image such that the difference between and the unknown ground truth is minimized. Typically, an LR image can be mathematically expressed as:
![]()
where denotes a blur operator, a downsampling function, and additive noise [21]. Recovering from is inherently ill-posed since multiple HR images can correspond to the same LR input.

Figure 2. Taxonomy of super-resolution (SR) techniques, categorized into video and image SR. Image SR further includes single-image and multi-frame SR approaches, encompassing reconstruction-, example-, sparse representation-, regression-, and deep learning-based methods.
Terminology.
In the super-resolution (SR) literature, the upscaling factor refers to the magnification ratio between low-resolution (LR) and high-resolution (HR) images, commonly ×2, ×4, or ×8 [13]. Single Image Super-Resolution (SISR) uses one LR input, whereas Multi-Frame Super-Resolution (MFSR) leverages multiple temporally or spatially aligned LR images [22]. Reference-based SR (RefSR) integrates external high-quality images as guidance, and Video SR (VSR) exploits temporal continuity.
Evaluation of super-resolution (SR) performance is commonly based on Peak Signal-to-Noise Ratio (PSNR) and Structural Similarity Index (SSIM) [gu27]. However, in medical imaging, these metrics may not accurately reflect clinical utility. Perceptual metrics such as LPIPS and task-based evaluations like segmentation accuracy or radiomic stability are increasingly being used [28].
Notational Conventions.
Let X ∈ ℝ h*w denote a low-resolution (LR) image and Y ∈ ℝ h*w the corresponding high-resolution (HR) image, with H = s × h and W = s × w, where s is the scaling factor. The SR mapping function fθ, parameterized by θ, is learned to minimize:
![]()
where Ŷ is the reconstructed high-resolution image.
Evaluation metrics play a critical role in measuring the performance of super-resolution (SR) algorithms. They determine not only the fidelity of the reconstructed image but also its perceptual and clinical utility. In medical imaging, choosing appropriate evaluation criteria is especially important because purely numerical improvements may not translate to better diagnostic outcomes [27].
Peak Signal-to-Noise Ratio (PSNR).
PSNR is the most widely used quantitative metric in image super-resolution (SR) tasks. It measures the pixel-wise difference between the reconstructed SR image (Ĩ) and the reference high-resolution (HR) image (I). It is defined as:
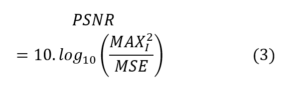
where MAX is the maximum possible pixel value, and MSE denotes the mean squared error. A higher PSNR indicates a lower reconstruction error [27]. Although PSNR is simple and easy to compute, it correlates poorly with perceptual quality in medical imaging scenarios.
Structural Similarity Index (SSIM).
SSIM measures perceptual similarity between two images by considering luminance, contrast, and structural information [27]. It is defined as:
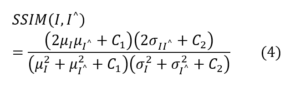
where μ and σ represent the mean and standard deviation, and C₁, C₂ are stability constants. SSIM better captures structural details than PSNR, which is important for detecting small lesions or anatomical features.
Learned Perceptual Image Patch Similarity (LPIPS).
LPIPS evaluates perceptual similarity using deep neural network features [26]. It compares feature activations between I and Ĩ using a pretrained network such as VGG. LPIPS correlates better with human perception [100] than PSNR or SSIM, making it valuable for evaluating perceptual quality in super-resolution (SR), especially when GAN-based methods are used.
Mean Opinion Score (MOS).
The Mean Opinion Score (MOS) is a subjective evaluation metric that involves radiologists or experts rating image quality on a predefined scale (for example, 1 to 5) [1]. It reflects clinical acceptability more accurately than objective metrics but requires human effort and standardized evaluation protocols. MOS is often used in validation studies of super-resolution (SR) algorithms for CT, MRI, and pathology images.
Perceptual and Fidelity Trade-offs.
Objective fidelity metrics such as PSNR and SSIM may not always align with perceptual or clinical image quality. GAN-based super-resolution (SR) methods often achieve lower PSNR but higher MOS or LPIPS scores. Therefore, multiple complementary metrics are typically reported to capture different aspects of image quality [28].
Multi-Scale and Region-Based Evaluation.
In medical super-resolution (SR), evaluating specific regions of interest (ROI) such as tumors, vessels, or soft tissue is more meaningful than relying on global averages. Multi-scale SSIM or ROI-based PSNR can provide more clinically relevant insights [7].
Standardized Benchmarks.
To ensure comparability, standardized datasets and evaluation protocols are essential. While natural image super-resolution (SR) has established benchmarks such as Set5, Set14, and DIV2K, medical SR requires modality-specific benchmarks for MRI, CT, ultrasound, and pathology [6].
Visualization and Qualitative Evaluation.
Figures and visual inspections are often used alongside quantitative metrics to highlight improvements in edges, textures, and lesion visibility. High perceptual quality is particularly important in clinical decision-making, even when numerical metrics are not optimal [26].
Recent studies have explored integrating both perceptual and clinical utility into the evaluation of super-resolution (SR) methods. Hybrid metrics that combine fidelity, perceptual similarity, and task-based outcomes are being developed to provide a more robust and clinically meaningful assessment of medical SR performance [28].
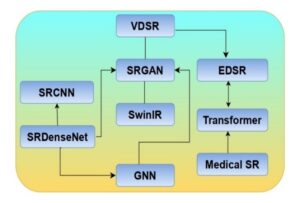
Figure 3. Evolution of deep learning-based super-resolution (SR) models, illustrating the progression from early CNN architectures (SRCNN, SRDenseNet, VDSR) to advanced frameworks (SRGAN, EDSR, SwinIR, Transformer, and GNN), culminating in specialized medical SR applications.
A fair and systematic comparison of super-resolution (SR) architectures is essential for understanding their relative strengths and limitations. In both natural and medical imaging, the performance of SR algorithms is typically evaluated using quantitative metrics such as Peak Signal-to-Noise Ratio (PSNR), Structural Similarity Index (SSIM), and Learned Perceptual Image Patch Similarity (LPIPS), along with qualitative assessments [28].
Benchmark Datasets.
Natural image super-resolution (SR) has well-established benchmark datasets such as Set5, Set14, BSD100, and DIV2K. These datasets provide standardized low-resolution (LR) and high-resolution (HR) pairs, along with defined degradation models, enabling consistent model evaluation [13].
In contrast, medical SR involves modality-specific datasets such as MRI brain images, low-dose CT datasets [95], and high-frequency ultrasound volumes [7] white matter tracts and small lesions. These datasets vary in resolution, noise characteristics, and clinical context, requiring specialized evaluation protocols and careful interpretation of quantitative metrics.
SR in Magnetic Resonance Imaging (MRI)
Magnetic Resonance Imaging (MRI) provides exceptional soft tissue contrast but is often acquired at lower resolution to reduce scan time and mitigate patient discomfort. Super-resolution (SR) reconstruction enables the enhancement of through-plane resolution, reduction of scan time, and improved depiction of anatomical details such as white matter tracts and small lesions [4].
Deep learning-based SR has been successfully applied to accelerate MRI protocols, producing diagnostic-quality images with significantly reduced acquisition times. Transformer-based SR methods [16] further improve structural fidelity across slices, supporting more accurate segmentation, quantitative analysis, and radiomic feature extraction in clinical workflows.
SR in Computed Tomography (CT)
Computed Tomography (CT) involves the use of ionizing radiation, making the trade-off between resolution and radiation dose clinically critical. Super-resolution (SR) enables the reconstruction [20] of high-resolution (HR) CT images from low-dose acquisitions, thereby reducing patient exposure while maintaining diagnostic quality [3].
GAN-based SR approaches have demonstrated superior performance in enhancing edge sharpness and lesion detectability, particularly in lung nodule screening and cardiac imaging [98]. Furthermore, SR can assist in recovering fine vascular structures and improving image quality for accurate radiotherapy planning.
SR in Ultrasound Imaging
Ultrasound is a real-time and low-cost imaging modality but suffers from low spatial resolution due to transducer and hardware limitations. Super-resolution (SR) techniques enhance ultrasound resolution, enabling improved visualization of microvascular structures, small lesions, and fetal anatomical details [5].
Recent advancements have introduced real-time SR models capable of running on edge devices, making them highly suitable for point-of-care and telemedicine applications. In addition, transformer-based and hybrid network architectures are being explored to achieve robust SR performance under challenging conditions such as speckle noise and motion artifacts.
SR in Digital Pathology and Microscopy
Digital pathology and microscopy produce gigapixel-scale images; however, high-resolution imaging is often expensive and time-consuming. Super-resolution (SR) enables the upscaling of lower-resolution scans while preserving fine cellular and subcellular details, thereby allowing faster slide scanning and efficient computational analysis [34].
Deep learning-based SR methods have been successfully applied in hematology, oncology, and histopathology workflows, supporting AI-driven diagnosis, biomarker quantification, and automated grading systems. These advancements enhance both the speed and accuracy of digital pathology pipelines in clinical and research environments [35].
SR for Functional and Dynamic Imaging
Super-resolution (SR) is increasingly being applied in functional MRI (fMRI), dynamic contrast-enhanced MRI, and 4D CT to address the trade-off between spatial and temporal resolution. By enhancing spatial resolution post-acquisition, SR enables shorter scan times while preserving essential functional and physiological information. This capability is particularly valuable in cardiac imaging, perfusion studies, and neuroimaging research, where temporal precision and anatomical detail are both crucial.
SR for Segmentation, Detection, and Radiomics
Super-resolution (SR) serves as a powerful preprocessing step to enhance downstream artificial intelligence (AI) tasks such as segmentation, registration, and classification. Higher-resolution images improve boundary delineation, particularly in tumor segmentation, vessel analysis, and organ contouring. In addition, SR contributes to more stable and reproducible radiomic feature extraction, which is highly sensitive to image resolution and voxel size [8].
Edge Deployment and Real-Time Applications
Lightweight convolutional neural network (CNN) and efficient Transformer models have made it possible to perform super-resolution (SR) in real-time clinical environments. These advancements enable SR on portable ultrasound devices, intraoperative surgical guidance systems, and low-resource medical setups. Such real-time implementations improve accessibility and accelerate clinical decision-making, particularly in emergency care and rural healthcare settings where computational resources are limited.
Applications in Medical Imaging.
Sparse coding methods were widely applied in Magnetic Resonance Imaging (MRI), Computed Tomography (CT), and microscopy-based super-resolution (SR) before convolutional neural networks (CNNs) [85][86] became dominant in the field. These methods improved through-plane resolution, edge sharpness, and noise suppression in reconstructed images while remaining computationally efficient compared to early deep learning models [41].
Limitations
Despite their strong performance, sparse coding methods rely heavily on handcrafted features, are sensitive to the quality of the learned dictionary, and often lack generalization to unseen domains. These limitations paved the way for deep learning-based approaches that automatically learn hierarchical feature representations directly from data.
Manifold Learning & Patch-Based ML Methods
Manifold learning-based super-resolution (SR) approaches assume that low-resolution (LR) and high-resolution (HR) image patches lie on low-dimensional manifolds embedded within high-dimensional spaces [47][42]. The key concept is to learn the intrinsic structure of these manifolds and utilize it to reconstruct HR patches from their LR counterparts. Unlike classical interpolation or linear regression approaches, manifold learning methods better preserve structural relationships, making them particularly effective for medical images that contain complex anatomical patterns and textures.
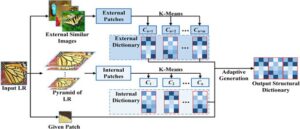
Figure 4. Illustration of an adaptive structural dictionary learning framework, where both internal and external patches are extracted and clustered using K-means to form internal and external dictionaries. These are then adaptively fused to generate an optimized output structural dictionary for image super-resolution.
Motivation
Medical images often contain highly structured patterns such as vessels, organ boundaries, and tissue textures that can be more effectively represented on nonlinear manifolds. Mapping low-resolution (LR) patches to high-resolution (HR) manifolds enables super-resolution (SR) algorithms to leverage geometric relationships rather than relying solely on pixel intensity similarity [43].
Locally Linear Embedding (LLE) for SR.
Chang et al. [43] introduced manifold learning into super-resolution (SR) through the concept of locally linear embedding (LLE). Given a low-resolution (LR) image patch, its k nearest neighbors is identified within the training dataset, and reconstruction weights are computed accordingly. The same weights are then applied in the high-resolution (HR) manifold to reconstruct the HR patch, as defined by the following equation:
Laplacian Eigenmaps
Belkin and Niyogi [48] proposed the Laplacian Eigenmaps method for manifold embedding, which preserves neighborhood relationships within a low-dimensional space. When applied to super-resolution (SR), this approach improves structural consistency between low-resolution (LR) and high-resolution (HR) image patches, resulting in better preservation of anatomical features and fine textures.
Manifold Alignment and Mapping.
More advanced super-resolution (SR) methods learn explicit mappings between low-resolution (LR) and high-resolution (HR) manifolds by aligning their geometric structures. This alignment can be achieved using techniques such as kernel regression, manifold alignment, or graph embedding approaches [47]. These methods enhance the ability of SR models to preserve structural coherence and spatial relationships across image scales.
Patch-Based Manifold SR
Patch-based ML models combine manifold learning with patch clustering or anchor-based selection to improve efficiency. In this framework, LR patches are embedded in a low-dimensional manifold, neighbors are selected, and corresponding HR patches are reconstructed through weighted combinations or learned mappings.
Manifold Learning in Medical SR.
Manifold learning methods have been applied to medical super-resolution (SR) to enhance Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) scans, particularly for improving through-plane resolution and preserving anatomical structure. Because these methods model local geometric relationships, they can handle anatomical variability
more effectively than traditional interpolation-based approaches [51][44].
Limitations.
Manifold-based super-resolution (SR) methods require large and diverse training datasets, are sensitive to neighbor selection, and often struggle to generalize to unseen anatomical patterns. In addition, these methods involve computationally expensive nearest-neighbor searches, which limit their scalability. These challenges ultimately led to the adoption of deep learning approaches that can learn complex nonlinear mappings directly from data.
Hybrid ML + Model-Based Reconstruction
Hybrid super-resolution (SR) methods combine model-based image reconstruction with machine learning (ML) priors to achieve improved image quality, better generalization, and enhanced stability [53][45]. These approaches integrate explicit imaging models—such as blur, noise, and down sampling functions—with learned patch-based or manifold-based priors. By doing so, they effectively bridge the gap between traditional inverse problem formulations and modern data-driven learning frameworks.
Motivation.
Pure model-based reconstruction methods rely on analytical priors such as total variation (TV) or edge-preserving regularization, which can over smooth important anatomical structures. On the other hand, purely machine learning-based methods may hallucinate or generate non-physical details that compromise clinical reliability. Hybrid approaches combine the strengths of both paradigms, ensuring physical consistency while enhancing perceptual and diagnostic image quality [11][46].
General Formulation.
Hybrid super-resolution (SR) methods are typically formulated as an optimization problem:
![]()
where x denotes the low-resolution (LR) image, H represents the imaging degradation model (such as blur and down sampling), and R(y) is a regularization term that incorporates learned priors—such as sparse coding, manifold structure, or regression-based constraints.
Patch-Based Learning Priors.
One hybrid approach integrates sparse coding priors into the reconstruction process. For instance, Elad and Aharon [40] incorporated dictionary learning into total variation (TV)-regularized reconstruction, enabling the preservation of fine structural details while maintaining strong data fidelity constraints.
Manifold and Regression Priors.
Protter et al. [53] proposed the use of neighbor embedding priors within a reconstruction framework for super-resolution (SR). In this approach, regression functions learned offline are combined with a forward imaging model to ensure that the reconstructed high-resolution (HR) output, when degraded, remains consistent with the original low-resolution (LR) input.
Regularization Techniques.
Hybrid super-resolution (SR) methods often incorporate total variation (TV) regularization, sparsity constraints, or edge-preserving priors alongside learned data-driven priors. This combination is particularly effective in medical imaging [99] applications, where it is crucial to preserve both smoothness and anatomical structures while enhancing fine details [22].
Applications in Medical Imaging.
In Magnetic Resonance Imaging (MRI), hybrid reconstruction techniques improve through-plane resolution by embedding machine learning (ML) priors into iterative reconstruction algorithms. In Computed Tomography (CT), these approaches are used to recover sharp structural details while effectively controlling noise [23][50]. Such methods are particularly attractive in scenarios where large training datasets are unavailable, as the model-based components contribute to improved stability and robustness.
Advantages and Limitations.
Hybrid super-resolution (SR) methods offer superior fidelity, interpretability, and stability compared to purely learning-based approaches. However, their iterative reconstruction procedures can be computationally expensive and are often sensitive to hyperparameter settings. These limitations inspired the development of later deep learning models, such as model-based deep unfolding networks [87][88], which build upon the foundational principles of hybrid SR.
Limitations of ML Methods in Medical Imaging
While classical machine learning (ML) methods for super-resolution (SR)—such as dictionary learning, regression-based mapping, and manifold learning—laid the groundwork for modern deep learning approaches, they exhibit several key limitations when applied to medical imaging [19]. These limitations arise from both methodological constraints and the inherent complexities of clinical imaging domains.
ML methods typically rely on handcrafted features, shallow regression models, or linear mapping functions. These are often insufficient to capture the rich anatomical variability present in medical images, particularly for complex modalities such as MRI and CT [10].
Medical data are heterogeneous across scanners, hospitals, and acquisition protocols. Models trained on one dataset often fail to generalize to others due to domain shift. Traditional ML models lack domain adaptation and transfer learning capabilities [22].
Dictionary learning and regression-based SR approaches require high-quality paired low-resolution (LR) and high-resolution (HR) datasets or large patch dictionaries. This is particularly challenging in medical imaging, where true HR ground truth data are not always available [12][49][85].
Most ML-based SR methods treat feature extraction, mapping, and reconstruction as separate modules. This modularity often leads to suboptimal results compared to deep learning methods that learn hierarchical features through end-to-end training.
Patch search, sparse coding, and neighbor embedding techniques require computationally expensive nearest-neighbor searches and optimization during inference [43]. This significantly limits their clinical applicability, especially in time-sensitive workflows such as intraoperative imaging.
ML-based SR methods often amplify acquisition noise or fail to handle motion artifacts due to their reliance on fixed linear mappings or local patch similarity [37][52].
Although ML methods are simpler than deep learning approaches, many still lack formal clinical validation and standardized reconstruction quality assurance protocols. This limits their acceptance in regulated clinical environments [36].
Most traditional ML methods ignore the forward imaging model, resulting in reconstructions that are not physically consistent with scanner acquisition models. This limitation is particularly problematic in CT imaging, where dose constraints and artifact suppression are critical [54][38].
As image sizes and modalities increase (for example, 3D MRI and 4D fMRI), the scalability of patch-based ML methods becomes a bottleneck. Storage requirements and computation time grow rapidly with dictionary size and neighbor searches.
Due to the aforementioned limitations, very few ML-based SR methods have achieved clinical translation or regulatory approval. Most remain confined to research or proof-of-concept studies rather than routine diagnostic workflows.
Deep learning (DL) has revolutionized image super-resolution (SR) by enabling the learning of complex nonlinear mappings from low-resolution (LR) to high-resolution (HR) images directly from data [14][39]. Unlike classical machine learning (ML) methods that depend on handcrafted features or shallow regression mappings, DL architectures can automatically learn hierarchical feature representations through multi-layer neural networks. This data-driven capability allows DL-based SR models to capture intricate spatial dependencies and recover fine anatomical details that are often lost in traditional reconstruction or interpolation techniques.
This section provides a concise background on the core building blocks used in modern SR architectures, focusing on neural network components, activation functions, and up sampling mechanisms.
Network Components
Most deep learning-based SR networks are composed of fundamental components such as convolutional layers, activation functions, normalization layers, and up sampling operators. These components form the backbone of SR architectures like SRCNN, VDSR, EDSR, SRGAN, and SwinIR.
Convolutional layers form the core building blocks of super-resolution (SR) networks. They extract local image features using learnable filters and shared weights, which enable translation-invariant feature extraction across the image. When multiple convolutional layers are stacked, the network progressively learns more abstract and complex feature representations, improving its ability to reconstruct fine details and textures [55].
Nonlinear activation functions such as ReLU, PReLU, and Leaky ReLU introduce nonlinearity into neural networks, allowing them to learn and approximate complex mappings between low-resolution (LR) and high-resolution (HR) representations. Among these, the Rectified Linear Unit (ReLU) is the most widely used due to its simplicity, effectiveness in mitigating vanishing gradients, and computational efficiency [57].
Batch Normalization (BN) and Instance Normalization (IN) are commonly used to stabilize network training and accelerate convergence by normalizing intermediate feature maps. However, some super-resolution (SR) networks—such as the Enhanced Deep Super-Resolution (EDSR) model—intentionally omit normalization layers to better preserve fine image details and avoid over-smoothing [59].
Residual connections enhance gradient flow and allow for the training of deeper neural network architectures without suffering from vanishing gradient problems. They are a fundamental component of modern super-resolution (SR) networks such as the Very Deep Super-Resolution (VDSR) and Enhanced Deep Super-Resolution (EDSR) models, enabling stable optimization and improved reconstruction performance [30].
Upsampling plays a critical role in super-resolution (SR) by reconstructing high-resolution (HR) images from low-resolution (LR) feature representations. Common upsampling strategies include:
Skip connections transmit low-level feature information to deeper layers, helping preserve fine image details and improving gradient flow during training. Dense blocks, as introduced in architectures such as DenseNet and SRDenseNet, further enhance feature reuse and encourage efficient information propagation across layers, resulting in better reconstruction quality and network stability [32][60].
Channel and spatial attention modules enable the network to focus selectively on the most informative regions and feature channels, thereby improving perceptual quality and reconstruction accuracy. These mechanisms help super-resolution (SR) models emphasize clinically relevant image areas while reducing redundancy in feature learning [26][61].
Although discussed in detail in later sections, it is important to note that deep learning-based super-resolution (SR) models typically employ a combination of loss functions to guide reconstruction quality. These include pixel-wise losses such as Mean Squared Error (MSE), perceptual losses that capture visual fidelity, adversarial losses used in Generative Adversarial Networks (GANs), and task-specific losses designed for clinical objectives such as segmentation or detection accuracy.
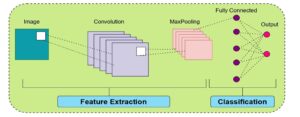
Figure 5. General architecture of a convolutional neural network (CNN), illustrating the feature extraction phase using convolution and max-pooling layers, followed by a fully connected network for classification and output prediction.
Convolutional Neural Networks (CNNs)
CNNs form the backbone of most deep learning-based super-resolution (SR) architectures. They are highly effective in modeling local spatial dependencies and learning hierarchical feature representations from image data, making them particularly suitable for reconstructing fine anatomical structures in medical imaging [55][62].
Core Principle.
Convolutional Neural Network (CNN)-based super-resolution (SR) models learn a nonlinear mapping function between low-resolution (LR) and high-resolution (HR) images. This can be mathematically expressed as:
![]()
where x denotes the LR input, ŷ represents the reconstructed HR image, and θ corresponds to the learnable network parameters. Stacked convolutional layers progressively extract hierarchical features from the input, enabling the network to recover fine details and enhance overall image fidelity.
Representative CNN SR Models
SRCNN [56]: The first CNN-based super-resolution (SR) model, consisting of a three-layer network that performs patch extraction, nonlinear mapping, and image reconstruction.
VDSR [30]: A very deep SR model that incorporates residual learning to enable stable optimization and faster convergence.
EDSR [15]: An enhanced deep SR network that removes batch normalization layers to produce sharper and more detailed images.
SRDenseNet [101]: Utilizes densely connected convolutional layers to encourage feature reuse and improve gradient propagation throughout the network.
Generative Adversarial Networks (GANs)
GANs have greatly improved the perceptual quality of super-resolution (SR) reconstructions by learning to generate realistic textures and fine details. Through the adversarial learning framework, GAN-based SR models encourage the generator to produce high-resolution images that are perceptually indistinguishable from real images [64][69].
GAN Structure
A Generative Adversarial Network (GAN) consists of two primary components: a generator (G) that reconstructs high-resolution (HR) images from low-resolution (LR) inputs, and a discriminator (D) that distinguishes real HR images from generated ones. The training objective is formulated as:
In this framework, the generator aims to produce realistic HR images that can “fool” the discriminator, while the discriminator learns to differentiate between genuine and generated samples. This adversarial training process drives the generator toward producing perceptually convincing images.
SRGAN [14] introduced adversarial training for super-resolution (SR), significantly improving perceptual sharpness and visual realism in reconstructed images.
Variants.
ESRGAN [29]: Incorporates enhanced perceptual loss and a relativistic discriminator to produce finer textures and improved detail consistency.
pGAN [65]: Applied to Magnetic Resonance Imaging (MRI) super-resolution, leveraging adversarial learning for high-quality image reconstruction.
CycleGAN: Enables unpaired SR learning by translating between low-resolution and high-resolution domains without requiring paired datasets.
Advantages.
Generative Adversarial Networks (GANs) are capable of producing sharp, realistic, and perceptually convincing images. They are widely adopted in medical super-resolution (SR) applications such as Magnetic Resonance Imaging (MRI) reconstruction, Computed Tomography (CT) [89] denoising, and digital pathology image enhancement, where high visual fidelity is crucial for accurate diagnosis.
Limitations.
Despite their effectiveness, GANs are challenging to train due to adversarial instability and sensitivity to hyperparameter selection. They may also hallucinate non-existent structures, which can compromise clinical reliability. Achieving a balance between perceptual sharpness and anatomical fidelity requires careful tuning of loss functions and training strategies.
Transformers and GNN/GCN
Recently, Transformer and Graph Neural Network (GNN) [17] models have demonstrated exceptional performance in super-resolution (SR) by capturing long-range dependencies and leveraging global contextual information [67].
Transformers in SR.
Transformers use self-attention mechanisms to model relationships between distant pixels, allowing them to reconstruct fine textures and maintain global image consistency. Architectures such as SwinIR [33] and IPT (Image Processing Transformer) [68] have achieved state-of-the-art performance in SR tasks, outperforming many convolution-based networks.
Advantages.
GNN/GCN in SR.
Graph Neural Network (GNN)-based SR methods represent image patches or anatomical regions as graph nodes. Graph convolution operations propagate information across these nodes, enabling efficient modeling of complex spatial relationships and irregular structures often found in medical images [80].
Applications.
Loss Functions Overview
Loss functions play a critical role in guiding super-resolution (SR) networks toward producing clinically meaningful reconstructions. In medical SR, a combination of pixel-wise, perceptual, and adversarial losses is often used to balance fidelity and visual realism [14][71].
Pixel-wise loss functions, such as Mean Squared Error (MSE) and L1 loss, are among the most commonly used in super-resolution (SR) tasks. They measure the average difference between the reconstructed high-resolution (HR) image and the ground truth image, ensuring pixel-level fidelity.
![]()
where yᵢ represents the ground truth HR pixel value, ŷᵢ is the corresponding reconstructed pixel value, and N is the total number of pixels. MSE emphasizes overall image fidelity but may produce overly smooth results, while L1 loss tends to preserve sharper edges.
Perceptual loss is computed based on deep feature representations extracted from a pre-trained network (such as VGG). It encourages perceptual similarity between the reconstructed and ground truth images, aligning them in feature space rather than relying solely on pixel-level accuracy [77][72].
Adversarial loss is used in Generative Adversarial Network (GAN)-based super-resolution (SR) models to enhance realism and texture quality. It helps the generator produce images that are perceptually closer to real high-resolution images [14].
Edge or gradient-based loss functions focus on preserving structural and textural details in images. They are particularly valuable in medical imaging for maintaining vessel boundaries, lesion edges, and other fine anatomical structures.
In medical SR applications, task-based loss functions are linked to specific downstream clinical objectives such as segmentation accuracy or disease classification performance [66]. This ensures that the reconstructed images are not only visually realistic but also clinically useful.
Modern SR networks typically use a combination of multiple loss functions to balance fidelity, perceptual quality, and realism. The total loss can be expressed as:
![]()
Machine learning (ML) and deep learning (DL) architectures form the foundation of super-resolution (SR) methods in medical imaging. While ML-based methods rely on handcrafted priors, patch similarity, and sparse representation, DL approaches learn hierarchical features end-to-end, enabling superior reconstruction quality. Hybrid methods combining both have recently emerged to leverage the advantages of each [74].
Table 1. Chronological Literature Review of Machine Learning–Based Medical Image Super-Resolution (2010–2019).
| No. | Author(s) | Year | Model / Method | Dataset/ Modality | Evaluation Metrics | Remarks / Future Scope |
|---|---|---|---|---|---|---|
| 1 | Jianchao Yang et al. | 2010 | Sparse Representation SR (coupled LR/HR dictionaries) | Natural images (Parthenon, Lena, Statue) | RMSE | Foundation for dictionary-learning SR; adapted later for MRI/CT |
| 2 | Van Reeth et al. | 2012 | MRI SR Survey (TV, Bayesian, POCS) | MRI phantoms and clinical datasets | PSNR, SSIM, SNR | Highlighted motion-free and anisotropic SR |
| 3 | Fang et al. | 2013 | SBSDI — Sparse Denoising + Interpolation for OCT | Retinal SDOCT (AREDS2) | PSNR, CNR | Introduced sparse priors for OCT SR; multimodal potential |
| 4 | Wang et al. | 2014 | Sparse Representation Reconstruction (SRR) for MRI | MRI sequences (Skull Base, Aorta, Knee) | PSNR | Proposed 3D SR with SSIM and clinical validation |
| 5 | Thapa et al. | 2014 | SR Algorithm Comparison for Retinal SR | Fundus images (Nidek AFC-230) | PSNR, SSIM | Suggested blind deconvolution and task-specific priors |
| 6 | Zhang et al. | 2015 | SRNINL — Sparse + Nonlocal MR SR | BrainWeb, ADNI | PSNR, SSIM | Nonlocal prior integration; improved computational efficiency |
| 7 | Tang et al. | 2015 | Sparse SR for Mass Spectrometry Imaging (MSI) | Rat brain (AFAI-MSI) | PSNR, RMSE | Introduced MSI SR; proposed 3D tissue-specific dictionaries |
| 8 | Wang et al. | 2015 | Dual Dictionary Learning (DDL) for Medical SR | CT, MRI datasets | PSNR, SSIM | Encouraged multimodal and physics-aware SR |
| 9 | Indu D. et al. | 2015 | Sparse SR for Fundus Fluorescein Angiography (FFA) | FFA clinical images (Amrita Institute) | Entropy, DIV | Used perceptual metrics; suggested GPU acceleration |
| 10 | Huynh et al. | 2016 | Structured RF + Auto-context for MR→CT SR | ADNI MR–CT paired scans | PSNR, MAE | Bridged MRI–CT SR; motivated hybrid RF–DL methods |
| 11 | Jog et al. | 2017 | REPLICA — Regression Ensembles for Contrast Agreement | Multi-contrast MRI (T1w, T2w, FLAIR) | PSNR, SSIM | Developed ensemble regression; potential hybrid CNN use |
| 12 | Zheng et al. | 2017 | Multi-contrast MRI SR (NEDI extension) | BrainWeb, real MRI | PSNR, RLNE | Extended NEDI with GPU optimization |
| 13 | Fang et al. | 2017 | SSR — Segmentation-based Sparse SR for OCT | Retinal SDOCT (41 subjects) | PSNR, CNR | Added shape-adaptive patches; cross-modality SR possible |
| 14 | Jiang et al. | 2018 | CT SR via Sparse Coding + Global Reconstruction | Dental CBCT, XCAT phantom | PSNR, SSIM | Validated feasibility of 3D SR in CBCT imaging |
| 15 | Wei et al. | 2018 | Multi-dictionary Sparse Coding + RF SR | MRI, CT (Siemens Gallery) | PSNR | Hybrid sparse + RF; proposed 4D SR |
| 16 | Abbasi et al. | 2018 | NWSR — Nonlocal Weighted Sparse SR for OCT | Retinal OCT (28 subjects) | PSNR, CNR, ENL | Improved denoising-integrated SR; GPU parallelization |
| 17 | Jiang et al. | 2018 | FFA SR Benchmark (10 SISR Algorithms) | Canon CF-60DSi Fundus images | PSNR, SSIM | Released FFA SR benchmark dataset |
| 18 | Dou et al. | 2018 | Random Forest Regression SR | MRI/CT datasets | PSNR, SSIM, runtime | Lightweight regression-based SR baseline |
| 19 | Zhang et al. | 2019 | MDL + NLSS SR | MRI, CT | PSNR, SSIM | Integrated deep priors with local self-similarity |
| 20 | Hu et al. | 2019 | PET SR via Coupled Dictionary Learning + RF | Whole-body PET lymphoma data | PSNR, SSIM, RMSE | 3D/4D PET SR; motion compensation with DL integration |
Table 2. Chronological Literature Review of Deep Learning–Based Medical Image Super-Resolution Methods (2016–2025).
| No. | Author(s) | Year | Model / Method | Dataset/Modality | Evaluation Metrics | Remarks / Future Scope |
|---|---|---|---|---|---|---|
| 1 | Jiwon Kim et al. | 2016 | VDSR (Very Deep Super-Resolution) | Set5, Set14, Urban100 (natural images) | PSNR, SSIM | Foundation for CNN-based SR; extendable to medical domains |
| 2 | Akshay S. Chaudhari et al. | 2018 | DeepResolve | Knee MRI (DESS) | PSNR, SSIM, MOS | Transferable to other MRI contrasts and anatomies |
| 3 | Honggang Chen et al. | 2018 | CISRDCNN | Set5, Set14 | PSNR, SSIM | Extend to compression and medical codec SR |
| 4 | Shengxiang Zhang et al. | 2019 | FMISR | Retinal DRIVE, Abdomen, Brain, Knee | PSNR, Runtime | Introduce GAN/perceptual losses; expand to 3D |
| 5 | Qing Lyu et al. | 2019 | GAN-CPCE / GAN-CIRCLE | IXI MRI | PSNR, SSIM | Scale to 3D GAN SR with improved realism |
| 6 | Chi-Hieu Pham et al. | 2019 | 3D CNN SR Network | Kirby 21, NAMIC MRI | PSNR, SSIM | Investigate perceptual SR and registration-free MRI SR |
| 7 | Tae-Hyung Kim et al. | 2020 | SRDenseNet for SISR | CDT Phantom (CT) | FWHM, CNR | Realistic CT validation with better spatial fidelity |
| 8 | Yuchong Gu et al. | 2020 | MedSRGAN | LUNA16 CT, Brain MRI | PSNR, SSIM, MOS | Extend to multimodal and Transformer-based SR |
| 9 | Yue Yu et al. | 2021 | WFSAN | Chest X-ray datasets | PSNR, SSIM | Integrate wavelet and frequency decomposition for SR |
| 10 | Zikang Wei et al. | 2021 | Improved SRGAN | DIV2K, Remote Sensing (RS) images | PSNR, SSIM | Lightweight design and multimodal adaptation |
| 11 | Heng-Sheng Chao et al. | 2022 | SRCNN/VDSR/EDSR for thin-slice SR | Clinical Chest CT | PSNR, SSIM | Extendable to other imaging modalities |
| 12 | Kejie Lyu et al. | 2022 | JSENet | MIT-Adobe FiveK dataset | PSNR, SSIM, LPIPS | Combine CNN and Transformer hybridization |
| 13 | Rui Cheng et al. | 2022 | FDSR | DIV2K, Set5 | PSNR, SSIM | Integrate domain-specific priors for medical SR |
| 14 | Waqar Ahmad et al. | 2022 | Progressive Multi-Scale GAN | Retinal, MRI, Ultrasound | PSNR, SSIM | Develop lightweight 3D SR architectures |
| 15 | Jay Shah et al. | 2024 | LDM-RR | ADNI, OASIS-3 (PET) | RC, SUVR | Optimize diffusion-based SR inference for PET imaging |
| 16 | Sevara Mardieva et al. | 2024 | DRFDN | DIV2K, Set5 | PSNR, FLOPs | Adapt to medical datasets and lower FLOPs |
| 17 | Alireza Esmaeilzehi et al. | 2025 | CLBSR | DIV2K, RealSR | PSNR, SSIM | Lightweight Transformer for Blind SR |
| 18 | Qiang Zhang et al. | 2025 | LRTENet | Hyperspectral datasets | PSNR, SSIM, SAM | Integrate global Transformer modules |
| 19 | Ke Xu et al. | 2025 | SCAN | DIV2K, Set5 | PSNR, SSIM | Edge deployment and knowledge distillation |
| 20 | Masuma Aktar et al. | 2025 | FA-PWSR | DIV2K, Set5 | PSNR, SSIM, LPIPS | Perceptual Transformer-based lightweight SR |
| 21 | Khushboo Singla et al. | 2025 | D-RRDN | CAMUS, LFW | PSNR, SSIM | Incorporate Transformer-based attention |
| 22 | Feiwei Qin et al. | 2025 | InfraFFN | IR700, FLIR (Infrared) | PSNR, SSIM | Lightweight FFN adaptation for IR SR |
| 23 | Garas Gendy et al. | 2025 | GMN | DIV2K, Set5 | PSNR, SSIM | Quantization and pruning for fast inference |
| 24 | Varsha Singh et al. | 2025 | MSARCNN | DIV2K, RealSR | PSNR, SSIM | Extend multi-scale CNN SR to medical domain |
| 25 | Shizhuang Weng et al. | 2025 | DWTN + AMResNet | Hyperspectral wheat data | PSNR, SSIM, ACC | Fusion of segmentation and RefSR methods |
Table 3. Chronological Literature Review of Deep Learning, GAN, and Transformer–Based Medical Image Super-Resolution Methods (2017–2025).
| No. | Author(s) | Year | Model / Method | Dataset/Modality | Evaluation Metrics | Remarks / Future Scope |
|---|---|---|---|---|---|---|
| 1 | Kenji Suzuki | 2017 | Overview of DL in Medical Imaging | CT, X-ray, MRI, PET | AUC, Sensitivity, Specificity, Dice | Lightweight DL, multimodal integration, clinical deployment |
| 2 | June-Goo Lee et al. | 2017 | DL in Medical Imaging: Review | CT, MRI, X-ray, PET | AUC, Dice, Accuracy | GANs, Transformers, self-supervised multimodal fusion |
| 3 | Dinggang Shen et al. | 2017 | Review of DL in Medical Image Analysis | MRI, CT, PET, Ultrasound | Dice, AUC, SSIM | Transformers, explainable AI, federated clinical DL |
| 4 | Yuhua Chen et al. | 2018 | DCSRN (3D Densely Connected SR Network) | HCP 3D MRI (T1-w) | PSNR, SSIM, NRMSE | Adversarial loss; hybrid Transformer SR |
| 5 | Justin Ker et al. | 2018 | DL Applications in Medical Imaging | CT, MRI, PET, X-ray, US | AUC, Dice, Accuracy | GANs/VAEs, lightweight transfer learning |
| 6 | Shengxiang Zhang et al. | 2019 | FMISR (Fast Medical Image SR) | Retinal DRIVE, Brain MRI, CT | PSNR, Runtime | GAN/Perceptual loss, 3D Transformer SR |
| 7 | Dwarikanath Mahapatra et al. | 2019 | P-SRGAN (Progressive GAN + Triplet Loss) | EYEPACS, Sunnybrook Cardiac MRI | PSNR, SSIM, AUC | Self-supervised, perceptual Transformer SR |
| 8 | Wenming Yang et al. | 2019 | DL for SISR: Review | DIV2K, Set5, Set14, Urban100 | PSNR, SSIM, LPIPS | Lightweight CNNs, realistic degradation modeling |
| 9 | Mingyu Kim et al. | 2019 | Deep Learning in Medical Imaging | X-ray, CT, MRI, PET | AUC, Sensitivity, Specificity | Unsupervised DL, Transformer fusion |
| 10 | Mohammad H. Hesamian et al. | 2019 | CNN, FCN, U-Net, V-Net | LUNA16, SLiver07, ISBI-2016 | Dice, IoU, Accuracy | Hybrid CNN–Transformer, unified benchmarks |
| 11 | Grant Haskins et al. | 2020 | DL for Image Registration: Survey | MRI, CT, US, X-ray, PET | TRE, DSC, MI, PSNR | Transformer/GAN for motion-aware registration |
| 12 | Chenyu You et al. | 2020 | GAN-CIRCLE | Tibia Micro-CT, Mayo Clinic CT | PSNR, SSIM, MOS | GAN + Transformer hybrid; adversarial robustness |
| 13 | Yabo Fu et al. | 2020 | DL in Medical Registration: Review | MRI, CT, US, PET | TRE, DSC, MI, PSNR | Transformer-based unsupervised registration |
| 14 | Yuchong Gu et al. | 2020 | MedSRGAN | LUNA16 CT, Brain MRI | PSNR, SSIM, MOS | GAN–Transformer hybrids; federated/self-supervised SR |
| 15 | Zhihao Wang et al. | 2021 | DL for Image SR (Survey) | DIV2K, Set5, ImageNet | PSNR, SSIM, LPIPS | Efficient GAN/Transformer hybrids for SR |
| 16 | Yutong Xie et al. | 2021 | CoTr (CNN + Transformer Hybrid) | BCV Abdominal CT (30 scans) | Dice coefficient | Joint segmentation–SR framework |
| 17 | Xiangbin Liu et al. | 2021 | FCN, U-Net, GAN, DeepLab, V-Net | MRI, CT, X-ray, US | Dice, IoU, Accuracy | Transformer integration, self-supervision |
| 18 | Yue Yu et al. | 2021 | WFSAN (Wavelet Frequency Separation Attention Net) | Chest X-ray (Shenzhen, Montgomery) | PSNR, SSIM | Multi-level wavelet + Transformer design |
| 19 | Waqar Ahmad et al. | 2022 | Multi-Path Progressive GAN | DRIVE, STARE, BraTS, CAMUS | PSNR, SSIM | Lightweight diffusion-based GAN SR |
| 20 | Heng-Sheng Chao et al. | 2022 | SRCNN, VDSR, EDSR for Thin-Slice SR | Chest CT (35 studies) | PSNR, SSIM | Cross-modality SR; add Transformers |
| 21 | Bai Zhengyao & Tao Jinyu | 2022 | P3DSRNet (Pseudo-3D SR) | Kirby-21 MRI | PSNR, SSIM, FLOPs | Extend to multi-modal SR |
| 22 | Defu Qiu et al. | 2023 | Survey: Medical Image SR Algorithms | MRI, CT, PET, US | PSNR, SSIM, MSE | Hybrid DL–GAN frameworks; lightweight SR |
| 23 | Hujun Yang et al. | 2023 | Review: Deep Learning in Medical SR | MRI, CT, PET, US | PSNR, SSIM, LPIPS | Transformer–GAN integration; perceptual metrics |
| 24 | Walid El-Shafai et al. | 2024 | SISR Review for Medical Imaging | COVID-CT, DRIVE, BraTS | PSNR, SSIM, FSIM | Real-time SR; lightweight GAN-Transformer |
| 25 | Shizhuang Weng et al. | 2025 | DWTN + AMResNet | Hyperspectral Wheat Dataset | PSNR, SSIM, ACC | RefSR + segmentation-aware fusion |
ML-Based Architectures
Early super-resolution (SR) in medical imaging relied on machine learning (ML) techniques such as dictionary learning, sparse coding, and regression-based mapping. These methods work well for structured anatomical patterns but often struggle with high variability and large-scale datasets.
Uses overcomplete dictionaries to reconstruct high-resolution (HR) patches from low-resolution (LR) inputs [33]. Widely used in early CT and MRI SR.
Formulates SR as sparse coding in a high-resolution dictionary space, enabling detail enhancement even with limited data.
Learn LR-to-HR mappings from paired patches (e.g., neighbor embedding, anchored regression).
Limitations:
DL-Based Architectures
Deep learning (DL) revolutionized medical super-resolution (SR) by enabling end-to-end learning of complex anatomical structures. Major architectural families include:
Examples include SRCNN, EDSR, and RCAN. These models are widely applied in CT, MRI, and ultrasound imaging.
SRGAN, ESRGAN, and pGAN improve perceptual quality and fine detail preservation [14].
Models such as SwinIR and IPT introduce global context modeling for large-scale medical images [33].
Graph convolutional networks leverage structural relationships across anatomical regions or patches.
Advantages:
Hybrid ML–DL Approaches
Hybrid super-resolution (SR) models combine the interpretability of machine learning (ML) with the representational power of deep learning (
]. Examples include:
Lightweight and Real-Time Models
Clinical deployment of super-resolution (SR) models requires low latency and high computational efficiency. Lightweight architectures are designed to minimize parameters and memory requirements without compromising reconstruction quality.
Strategies:
Network and Model Design Complexity
Modern super-resolution (SR) architectures such as Generative Adversarial Networks (GANs), Transformers, and Graph Neural Networks (GNNs) achieve state-of-the-art performance but introduce significant computational challenges. These include increased model size, complex training dynamics, and higher resource requirements.
Key Challenges:
Lightweight super-resolution (SR) models and neural architecture search (NAS) are promising directions for reducing computational complexity while maintaining high reconstruction accuracy [75].
Domain Shift and Generalization
Super-resolution (SR) models trained on one dataset often underperform when applied to data from different scanners, institutions, or patient populations. This domain shift arises due to variations in imaging protocols, noise characteristics, and anatomical structures [73].
Examples:
Domain adaptation, self-supervised learning, and harmonization techniques are promising solutions to mitigate domain shift and improve generalization across diverse clinical environments [70].
Real-World Deployment Challenges
Even high-performing super-resolution (SR) models face significant challenges when transitioning from research to clinical deployment:
Regulatory compliance [83]: FDA and EMA approvals require extensive validation and reproducibility studies.
Integration: Seamless interfacing with PACS, RIS, and scanner systems is essential for workflow compatibility.
Real-time requirements: Clinical environments demand low-latency inference for time-critical decision-making.
Interpretability and trust: Clinicians require explainable SR outputs to ensure diagnostic reliability.
Bridging the gap between laboratory performance and real-world clinical adoption requires close collaboration among researchers, clinicians, and industry partners [79].
Future Research Directions
Although deep learning has significantly advanced medical image super-resolution (SR), the field remains far from clinical maturity. Future research should emphasize data-efficient learning, robustness, explainability, an
d practical deployment.
Self-Supervised and Unsupervised SR
Traditional supervised super-resolution (SR) methods rely on paired low-resolution (LR) and high-resolution (HR) datasets, which are often difficult to acquire in medical imaging. Self-supervised [24] and unsupervised SR approaches [94] eliminate the need for ground-truth HR images by learning from internal image statistics or domain-specific priors.
Potential Benefits:
Applications include MRI reconstruction without paired datasets and pathology image enhancement using internal learning.
Domain Adaptation
Medical super-resolution (SR) models often fail to generalize under domain shift. Domain adaptation and generalization approaches [96] aim to make SR models robust across different scanners, imaging protocols, and patient populations.
Strategies:
Domain-adapted SR models will facilitate reliable deployment in multi-center studies and low-resource clinical environments.
Federated and Privacy-Preserving SR
Patient privacy and data governance are major challenges for large-scale super-resolution (SR) model training. Federated learning (FL) enables collaborative model training across multiple institutions without requiring centralized data sharing [84][76].
Key Advantages:
Future research should focus on integrating SR with federated learning and differential privacy techniques to support scalable and secure clinical deployment.
Multi-Task SR
Future super-resolution (SR) models are expected to integrate multiple related tasks such as segmentation, detection, or registration into a single framework. This multi-task learning approach can enhance both image reconstruction quality and downstream clinical performance [25][78].
Advantages:
Examples include joint SR with tumor segmentation in MRI or combining SR with registration for longitudinal imaging studies.
Efficient SR for Low-Resource Clinical Settings
Many hospitals, particularly in low-resource regions, lack access to high-end computing hardware. Designing efficient super-resolution (SR) architectures—such as lightweight CNNs, knowledge distillation, and quantized models—is crucial for practical, real-world adoption [73][81].
Future Focus:
Explainable SR Models
To gain clinical trust, super-resolution (SR) models must be interpretable and transparent. Explainable SR (XSR) techniques enable radiologists to understand how image details are reconstructed and validated
[73].
Key Directions:
These approaches will accelerate the acceptance of SR algorithms in regulated clinical workflows.
Medical image super-resolution (SR) has evolved from conventional interpolation and sparse-representation techniques to advanced deep learning paradigms, significantly enhancing spatial fidelity, structural consistency, and diagnostic reliability across imaging modalities. By reconstructing high-resolution details from low-quality acquisitions, SR contributes to faster scans, reduced radiation exposure, and improved clinical interpretability in MRI, CT, ultrasound, digital pathology, and PET/SPECT.
This survey has provided a comprehensive synthesis of medical image SR methodologies, encompassing foundational concepts, network architectures, benchmark datasets, and evaluation metrics. It systematically reviewed the progression from early CNN-based frameworks to advanced GAN-, Transformer-, and graph-based architectures, highlighting their strengths, limitations, and clinical implications. Comparative analyses revealed the trade-offs between visual fidelity, computational cost, and clinical relevance, while emphasizing the growing importance of hybrid and lightweight designs for practical deployment.
Despite remarkable progress, several challenges persist—most notably, limited availability of annotated medical datasets, privacy restrictions, cross-domain variability, interpretability concerns, and the absence of standardized evaluation protocols. Addressing these issues will be critical for bridging the gap between algorithmic innovation and real-world clinical integration.
Future research directions should emphasize:
Ultimately, the clinical translation of medical image SR will depend on cross-disciplinary collaboration among researchers, clinicians, and policymakers. Establishing unified benchmarking standards, rigorous validation pipelines, and interpretable SR frameworks will be essential for achieving regulatory acceptance and widespread adoption.
In summary, medical image SR represents a cornerstone of next-generation diagnostic imaging and precision medicine. With continuous advancements in algorithmic design, data governance, and clinical validation, SR is poised to become an indispensable component of future healthcare imaging ecosystems, enhancing both accessibility and quality of patient care.
